If you’re weighing the advantages and disadvantages of IVF, you’re probably deep in a hard decision, not casually browsing. Most people searching this term have already tried other paths or have just received a diagnosis that makes natural conception unlikely. Either way, you want a straight answer, not a sales pitch.
I’ll walk you through this the way I would with a patient across from me. We won’t just list the pros and cons of IVF and call it a day. Every benefit comes with a limit worth knowing, and every risk comes with real numbers, based on 2025-2026 data from the CDC, SART, and ASRM.
By the end, you should understand the actual benefits of IVF for your situation, the risks that matter most for your age and diagnosis, and whether the cost is likely worth it for you. This isn’t a decision anyone else can make for you, but it should be an informed one.
Advantages of IVF
Let’s see some advantages of IVF that can help you build a happy family:
High Success Rate
The science. IVF bypasses many barriers that block natural conception, such as blocked tubes, low sperm count, and ovulation disorders, by fertilizing the egg outside the body and placing the embryo directly into the uterus.
The real numbers. In 2026, women under 35 see live birth rates of roughly 40-50 percent per embryo transfer, women 35-37 see about 30-35 percent, and women 38-40 see roughly 20-25 percent. Cumulative rates after three complete cycles can reach 85 percent or higher under age 40.
The limit. These are averages across large groups, not guarantees. A single cycle is one attempt, and most patients who succeed need more than one try.
Works for Many Causes of Infertility
The science. Unlike treatments that target one specific problem, IVF can work around tubal damage, unexplained infertility, endometriosis, and both male and female factors at once.
The real numbers. IVF accounts for the majority of assisted reproductive technology cycles performed worldwide because of this flexibility.
The limit. IVF isn’t automatically the right first step for every diagnosis. Some causes respond just as well to simpler, cheaper treatments first.
Helps Male Infertility
The science. With intracytoplasmic sperm injection (ICSI), a single healthy sperm is injected directly into an egg, helping couples facing low sperm count, poor motility, or abnormal shape.
The real numbers. ICSI is used in the majority of IVF cycles involving any male factor diagnosis, with fertilization rates comparable to standard IVF even in severe cases.
The limit. ICSI improves fertilization rates but doesn’t fix underlying sperm DNA fragmentation, which can still affect embryo quality.
Helps Female Infertility
The science. IVF can work around blocked or damaged fallopian tubes, ovulatory disorders, and diminished ovarian reserve by retrieving eggs directly and controlling fertilization in the lab.
The limit. Severely diminished ovarian reserve still lowers the number of eggs retrieved, which can limit embryo count regardless of lab conditions.
Genetic Testing
The science. Preimplantation genetic testing (PGT-A) screens embryos for chromosomal abnormalities before transfer, lowering the chance of transferring an embryo likely to end in miscarriage.
The limit. It adds cost, typically $4,500-$10,000, and 2025 research found it doesn’t meaningfully improve cumulative live birth rates for every group, including some patients with recurrent pregnancy loss.
Fertility Preservation
The science. IVF technology allows eggs, sperm, or embryos to be frozen for future use, which matters for people delaying parenthood or facing medical treatments like chemotherapy that can affect fertility.
The limit. Freezing doesn’t guarantee future success; outcomes still depend heavily on the age at which eggs were frozen.
Frozen Embryos
The science. Frozen embryo transfer (FET) allows patients to use embryos from a single retrieval across multiple attempts, and current evidence suggests that a freeze-all approach can improve live birth rates by allowing the uterine lining time to recover from stimulation.
The limit. Frozen transfers add their own cost, typically $4,000-$6,400 per transfer, on top of the original retrieval.
Donor Eggs
The science. Donor egg IVF removes maternal age as the main limiting factor, since egg quality, not the recipient’s age, drives most of the outcome.
The real numbers. Success rates with donor eggs hold steady around 45-55 percent per transfer, largely independent of the recipient’s own age.
The limit. Donor egg programs add significant cost, often $15,000-$35,000, and raise personal and legal questions some patients need time to work through.
Donor Sperm
The science. Donor sperm allows conception for couples facing severe male infertility, single women, and same-sex female couples, using the same IVF or IUI process.
The limit. Cost per vial ranges from $400 to $2,000, and supply or matching preferences can add to waiting time.
Family Planning
The science. IVF gives patients more control over timing, including the ability to test embryos for known inherited conditions before pregnancy begins.
The limit. This level of control comes with real financial and emotional weight, worth planning for rather than underestimating.
Bottom line: the benefits of IVF are real and well documented, but each one comes with a caveat. None of them guarantees IVF; they make it a strong option worth fully understanding.
Disadvantages of IVF
Now, it turns to consider some disadvantages of IVF:
Cost
Cause. IVF requires specialized lab equipment, medications, and skilled staff for every cycle.
How often. Every patient faces this; it isn’t a rare complication, it’s a certainty of treatment.
Severity. In the United States, one cycle now averages roughly $15,000-$30,000 including medications, and most patients need two to three cycles, pushing total costs toward $50,000 or more.
Can it be reduced? Around 25 states now mandate some level of fertility insurance coverage as of 2026, and multi-cycle refund programs can lower risk, though only about a quarter of Americans currently have IVF insurance benefits.
IVF costs can be reduced if you choose to have it abroad; we mentioned the cheapest country for IVF if you want to do so.
Emotional Stress
Cause. The uncertainty of each cycle, the physical demands of injections, and the two-week wait before a pregnancy test all add up.
How often. Nearly universal; most patients describe this as one of the hardest parts of treatment, regardless of outcome.
Severity. Ranges from manageable anxiety to clinically significant depression, particularly after failed cycles.
Can it be reduced? Counseling support, realistic cycle limits set in advance, and connecting with others going through treatment all help.
Physical Side Effects
Cause. Hormone injections stimulate the ovaries to produce multiple eggs, which can cause bloating, mood swings, and injection-site soreness.
How often. Common in some degree for nearly all patients during stimulation.
Severity. Usually mild and temporary, resolving within days of egg retrieval.
Can it be reduced? Your care team can adjust medication dosing based on your response to lower discomfort.
Multiple Pregnancy
Cause. Transferring more than one embryo increases the odds that more than one embryo implants.
How often. Twin rates with double embryo transfer in women over 35 have been measured as high as 22-29 percent in some studies, compared with roughly 1-2 percent for single embryo transfer.
Severity. Twin and higher-order pregnancies carry a higher risk of premature birth and neonatal complications.
Can it be reduced? Yes, ASRM guidelines now recommend single-embryo transfer for most patients, specifically to avoid this risk.
OHSS (Ovarian Hyperstimulation Syndrome)
Cause. Fertility medications can overstimulate the ovaries, causing fluid shifts into the abdomen.
How often. Moderate-to-severe OHSS occurs in roughly 1-5 percent of IVF cycles overall, though risk climbs to around 20-25 percent in high-risk patients such as those with PCOS.
Severity. Mild cases cause bloating and discomfort; severe cases, occurring in roughly 0.1-2 percent of cycles, can require hospitalization.
Can it be reduced? Yes, modern GnRH-antagonist protocols and freezing all embryos instead of a fresh transfer both meaningfully cut OHSS risk. U.S. surveillance data show that OHSS rates have fallen from about 1.05 percent to 0.42 percent over the past decade as these protocols became standard.
Failed Cycles
Cause. Not every embryo implants, even when it looks healthy under the microscope.
How often. Even under age 35, a single cycle still carries roughly a 50-60 percent chance of not resulting in a live birth; odds improve with subsequent attempts.
Severity. Emotionally difficult, though a failed cycle does not mean subsequent attempts will fail too.
Can it be reduced? Genetic testing and optimized protocols can improve odds, though no clinic can eliminate this risk entirely.
Miscarriage
Cause. Chromosomal abnormalities remain the leading cause, and their frequency rises with maternal age regardless of conception method.
How often. National data puts miscarriage rates after IVF anywhere from 11-45 percent depending heavily on maternal age, with the higher end concentrated in patients over 40.
Severity. Physically manageable in most cases, but emotionally significant, especially after a positive pregnancy test.
Can it be reduced? Genetic screening of embryos before transfer can lower this risk for some patients, though not eliminate it.
Ectopic Pregnancy
Cause. Even though the embryo is placed directly in the uterus, it can still move into a fallopian tube before implantation, especially in patients with pre-existing tubal damage.
How often. Ectopic pregnancy occurs in roughly 1.5-2.1 percent of IVF pregnancies with single embryo transfer, rising toward 2.5 percent when more embryos are transferred.
Severity. Serious; ectopic pregnancies cannot continue safely and require prompt medical treatment.
Can it be reduced? Single embryo transfer measurably lowers this risk compared with transferring multiple embryos.
Time Commitment
Cause. A single cycle involves two to three weeks of monitoring appointments, injections, and procedures, and most patients need more than one cycle.
How often. Universal; there’s no shortcut around the monitoring schedule required for safety.
Severity. More disruptive for patients balancing full-time work or travel to a clinic.
Can it be reduced? Some clinics offer early morning monitoring hours, and minimal-stimulation protocols can shorten certain cycles.
These aren’t reasons to avoid IVF, but they are reasons to go in with your eyes open and a realistic sense of what a typical experience looks like.
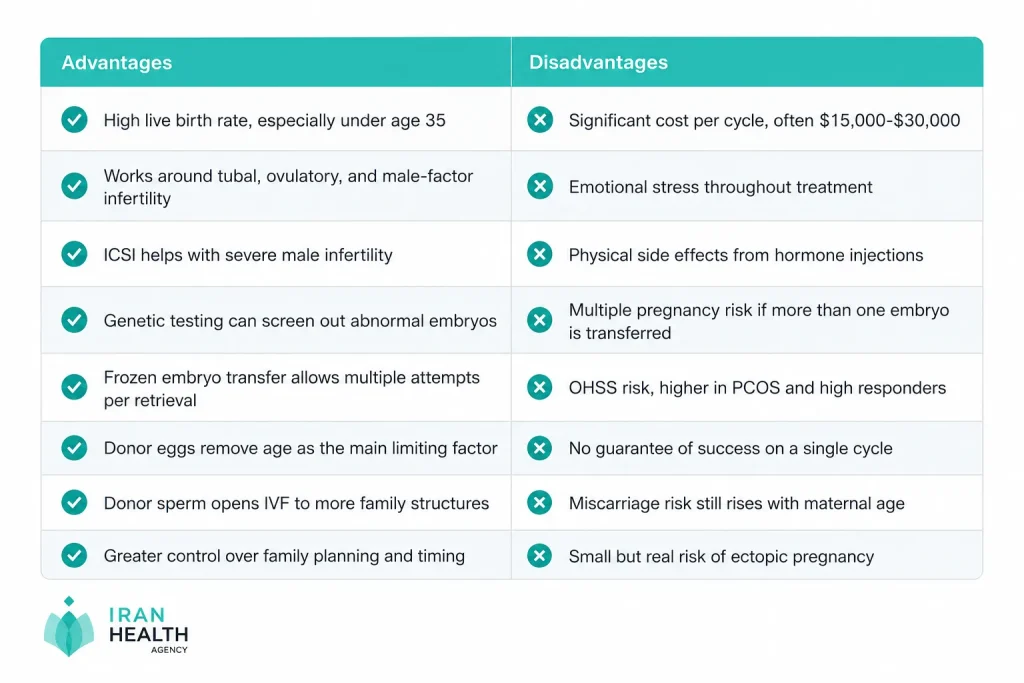
Pros and Cons Table
Here’s the full picture of IVF pros and cons, side by side, so you can weigh it in one glance.
Risks vs Benefits: Is IVF Worth It?
This is the question underneath every other question, and there’s no single answer that fits everyone.
If you’re under 35 with a clear diagnosis like blocked tubes, the statistics favor you: high per-cycle success rates and a strong cumulative chance across a few attempts. The benefits of IVF are especially strong here.
If you’re over 40 using your own eggs, the numbers shift. Per-cycle success rates drop into the teens or lower, and miscarriage risk rises. This doesn’t mean IVF won’t work, but the conversation should include donor egg options honestly, not as a last resort mentioned only after repeated failures.
If cost is your biggest concern, ask about multi-cycle refund programs and your state’s insurance mandate before assuming IVF is out of reach.
If emotional stamina is your biggest concern, set a clear plan in advance for example, a defined number of retrievals and transfers before reassessing so you’re making decisions in calm moments, not in the middle of a hard month.
Bottom line:
IVF tends to be worth it when your specific diagnosis, age, and finances line up with what the data shows works. A fertility specialist who reviews your actual labs, not just your age, is the only person who can translate these averages into your personal odds.
Free Consulation

Conclusion
Weighing the advantages and disadvantages of IVF isn’t about deciding whether IVF is good or bad; it’s a well-studied, effective treatment that has helped millions of families. It’s about whether it fits your specific age, diagnosis, budget, and emotional bandwidth right now.
If the benefits of IVF outweigh the disadvantages for your situation, it can be one of the most effective infertility treatments available. But that call shouldn’t be made from a blog post, including this one it should follow a full evaluation with a qualified fertility specialist who reviews your history, age, and specific cause of infertility.
If you’d like to talk through where you stand, our team offers a free consultation to walk through your options honestly, without pressure toward any particular path.

Frequently Asked Questions
What are the disadvantages of IVF?
Cost, emotional stress, physical side effects, and medical risks including OHSS, multiple pregnancy, miscarriage, and a small rise in ectopic pregnancy risk versus natural conception.
What is the biggest risk of IVF?
OHSS and multiple pregnancy carry the most clinical concern, though both are largely preventable with modern protocols and single embryo transfer.
What are the main benefits of IVF?
A comparatively high success rate for many infertility causes, the ability to screen embryos genetically, and flexible options like frozen embryos and donor eggs or sperm.
Is IVF painful?
Most discomfort comes from daily injections, not the procedures. Egg retrieval uses sedation, and embryo transfer typically causes minimal sensation.
How many IVF cycles does it usually take?
Most patients need two to three cycles, though cumulative success rates after three cycles can exceed 85 percent under age 40.
Does IVF increase the risk of birth defects?
Overall risk stays low, though some studies show a small increase versus natural conception, likely tied to underlying infertility factors rather than the IVF process itself.
Is IVF safe for older women?
Generally yes, but success rates drop, and miscarriage risk rises with maternal age, which is why donor egg options are often discussed for women over 40.
Can IVF fail even with a healthy embryo?
Yes. Implantation depends on more than embryo quality; the uterine environment and timing matter too, so genetically normal embryos don’t always result in a live birth.
Does IVF guarantee twins?
No, and modern guidelines discourage aiming for twins. Single embryo transfer is now recommended for most patients, specifically to avoid the added risks of a multiple pregnancy.
How much does IVF cost in 2026?
In the U.S., a single cycle typically costs $15,000-$30,000, including medications, with totals often reaching $50,000 or more across multiple cycles without insurance.
Who should consider a different treatment than IVF?
Patients with mild, unexplained infertility, especially younger women, may try simpler options like ovulation induction or IUI first, since IVF’s cost and intensity aren’t always necessary as a first step.
Sources
- CDC, “ART Success Rates” — https://www.cdc.gov/art/success-rates/index.html
- SART, “National Summary Report” — https://www.sartcorsonline.com/rptcsr_publicmultyear.aspx
- ASRM, “Prevention of Moderate and Severe Ovarian Hyperstimulation Syndrome: A Guideline (2023)” — https://www.asrm.org/practice-guidance/practice-committee-documents/prevention-and-treatment-of-moderate-and-severe-ovarian-hyperstimulation-syndrome-a-guideline/
- BJOG, “The Management of Ovarian Hyperstimulation Syndrome, Green-Top Guideline No. 5 (2026)” — https://obgyn.onlinelibrary.wiley.com/doi/10.1111/1471-0528.70195
- PMC, “Ovarian Hyperstimulation Syndrome (OHSS) Requiring ICU Admission, England/Wales/NI 1996-2020” — https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9797661/
- PMC, “Ectopic Pregnancy Rates with Day 3 versus Day 5 Embryo Transfer” — https://pmc.ncbi.nlm.nih.gov/articles/PMC270025/
- Carrot, “How Much Does IVF Cost in the U.S.?” — https://www.get-carrot.com/blog/ivf-cost-understanding-the-expenses-of-in-vitro-fertilization